This 16 year old girl is my hero. Impressed that she stood up to B.O. and confronted him about drone strikes.
 I recently joined a company called CrowdMed, which is a startup based in Silicon Valley that applies crowdsourcing to real medical mysteries. My role as a campus ambassador is to recruit MD's (at CrowdMed, MD means medical detective, which is typically a medical student or recent graduate from medical school). I will also be managing the social media, which is an extra responsibility, but something that I'm pretty pumped about doing. My sister works in social media marketing and has offered to teach me about strategy development. Looking forward to learning a lot on the job, and contributing to a company that is doing something cool and new.
I first became interested in the startup scene in March 2013, when I visited my buddy Mike Mayer in New Orleans. He gave me exposure to his startup in the Big Easy and invited me to join a design thinking workshop with his colleagues at Venture for America. This was a very interesting experience. While one dude prodded our brains for ideas, we put sticky notes on the wall and shifted around in desks that felt like spaceships. We did word association exercises and gave mini-presentations to each other on a variety of topics related to social entrepreneurship. The ideas that we were coming up with were insignificant, but our process of discovering ideas was the bee's knees. The VFA fellows were implementing paradigms that originated at a company called Ideo. From my understanding, Ideo is a company that re-evaluates methods, processes and structure for every possible facet of running a business. Without being facetious, this session was essentially a brainstorming exercise about brainstorming. It had me itching to figure out how it could be applied to medicine. CrowdMed is the first thing I've heard of that has invented a paradigm for helping patients who are very, very sick and haven't had a satisfactory diagnosis after seeing dozens of doctors. I'm optimistic about the prospects of CrowdMed and it's potential impact to prolong life, alleviate suffering and improve health. The academic demands of being an MSII have gotten the best of me lately and have limited me from writing verbose reflections. But, here are some notable articles that I enjoyed reading from this past week.  Shutdown coverage fails Americans Aljazeera America Dan Froomkin argues that our journalists should be shackled to political neutrality. Important perspective to keep in mind during the political snafu that is the ongoing federal government shutdown. My main takeaway from this story is that I wish that the fictional news anchor, Will McAvoy, from HBO's The Newsroom, was real.  What's In it: Doritos Locos Tacos NYTimes Aaron Byrd and Michael Moss take a serious look at a not-so-serious food item and explore the marketability and the science behind this Taco Bell delicacy.  From Therapy Dogs To New Patients, Federal Shutdown Hits NIH NPR Although the clinical research center at NIH is still up and running, many important services that patients rely on for treatment are not available for them. Also, new medical research in America is on hiatus across the country as Congress fails to make any progress on a resolution.  Pussy Riot Member Hunger Striking Over Brutal Prison Conditions Gawker
Nadezhda Tolokonnikova is fearlessly hunger-striking to call attention to inhumane conditions and cruel punishments in a Russian prison. As a trauma surgeon, Dr. Sarani is in a very good position to advocate for a reduction in gun violence. Read the story on MSCNBC. Also, a tip of the hat goes to my home state of Maryland, which is a safer place as a result of implementation of a new set of gun laws.  If you care about this stuff, check out Mayors Against Illegal Guns on Facebook for stats, infographs and the latest news on Michael Bloomberg's efforts to reduce gun violence.
Here are some of my goals from this past summer and elaborations on the challenges and successes related to accomplishing those goals.
Publish a paper in a peer-reviewed journal. This was probably the most cliché goal that a first year medical student could have, but I would be lying if I didn’t say that was the most important objective for my summer. I started off working on two separate projects this summer in order to hedge my bets and follow through with whichever paper had the best chance of getting published. This did not last very long. One mentor that I was working with (still working with?) has lofty goals of implementing a Zagat-style scoring for surgeons across all sub-specialties. I was impressed with the novelty of the idea and the proprietary interests that my mentor has, but we lost touch over the summer after he failed to follow up with my communications. I am still very interested in this project and continuing work on the literature review, but this project is tabled for the time being. My current work-in-progress is an 8,000 word literature review on assessments of male infertility in epidemiological research. This was the project that I was working on at NICHD. I am working with a third year Reproductive Endocrinology and Infertility (REI) fellow at NIH, an epidemiologist and the director of our branch to get this paper published. I do most of the work, with researching, writing and presenting. My clinical fellow provides me with feedback on a regular basis on how to edit and move forward. The epidemiologist and director check in with me at major milestones in my research process and give me valuable guidance with big-picture stuff. This research is very interesting to me. I have learned a lot about the field of infertility treatment, an area of medicine that I am particularly interested in. A major direct success of my research project was discussing a poster that summarized my findings to my department in a brief presentation and presenting my poster at the NIH summer student poster day- an event that a few of my other medical school colleagues in my class participated in. Gain clinical exposure in Reproductive Endocrinology. I had the chance to shadow reproductive endocrinologists on two occasions at the Clinical Center at NIH, which I thoroughly enjoyed. I was challenged by the clinical fellows with topics in female reproductive physiology and had the chance to observe clinical consults. I also attended various clinical seminars at NIH on topics such as PCOS, premature menopause and other REI subjects. Earlier in the summer, I observed egg retrievals and other laboratory procedures at an In-Vitro Fertilization clinic in Puerto Rico. Attend various seminars and journal clubs. As part of my summer student experience in the Division of Intramural Population Health research, I participated in a summer student course, which was taught by the post-doctoral research fellows. Topics ranged from biostatistics, epidemiological research methods and how to publish a paper. I also participated in a weekly journal club, and gave a presentation on an ethical research dilemma involving varying oxygen levels in a study design involving newborn infants. This was a particularly rewarding experience, because I had the opportunity to facilitate a discussion among a particularly diverse group of pre-doctoral and post-doctoral experts from various backgrounds. I was occasionally the person to give clinical insight into research discussions during seminars and journal clubs as I was frequently the only person in the room who had any sort of clinical experience. The seminars at NIH were simply incredible. Having the opportunity to listen to the most current research from the experts in their respective fields was awesome. I attended a presentation given by someone at the Office of Scientific Research at the White House who was pitching potential ideas for collaboration between NICHD and the White House and discussed initiatives for incorporating big data into research. I listened to a basic science researcher discuss his research on ovarian cancer in Drosophila flies. I also heard about research on maternal health in Argentina, which was an impressive presentation given by an international collaborative research team. Learning by osmosis was huge for me this summer, but I took the opportunity to challenge myself with understanding as much material as I could and ask questions whenever it was appropriate. Establish professional relationships with co-interns and employees. Networking at NIH was important to me, and it is something that I’ve taken seriously since I listened to a seminar given by Keith Ferrazzi, the author of Never Eat Alone. Over the course of the summer, I ate lunch, drank responsibly at happy hours and displayed masterful culinary skills at potluck events with my co-interns. And nearly every day, I worked out in a local park for a half-hour with my boss and other staff employees. These informal interactions with my co-workers were integral components of making my work experience enjoyable. They also solidified my relationships with these people for maintaining professional relationships in the future. I also formally networked and established contact with some important administrators at NICHD. I had lunch with the deputy director of extramural research, Dr. Caroline Signore, who is also a GWU graduate student alum. I got to hear about her career in OB/GYN and NICHD. I bounced ideas off of Dr. Stuart Moss, the director of intramural research in male infertility at NICHD and learned about current research in male infertility and shared with him my results from my research project. Stay intellectually stimulated. I wanted to work out my brain this summer in a different way than med school keeps my brain fit. Combing through Pubmed on a daily basis and learning about epidemiology research and biostatistics expanded my framework for thinking about medicine. I appreciate the different bits of knowledge I picked up on those domains this summer. I also began writing a blog this summer to start to formalize my thoughts on healthcare and share them with my friends and family. I also designed this blog to develop my brand as a future physician, something I consider to be important to me. You can read my blog at neildubey.weebly.com Understand how a large research institution functions. This was a very interesting aspect of my internship experience. As a summer student, I got the inside perspective into how people from various expertise can work together to conduct research. A unique way I learned about this was sitting in on weekly conference calls for a clinical trial that my department was conducting in Minnesota and Utah. Learning about the logistics of collecting data and managing thousands of patients was slightly overwhelming, yet very interesting. Observing how my department director troubleshooted, managed a team and delegated tasks was an important lesson in management skills and something I paid attention to in our department meetings. General Reflections I could not have imagined a better summer experience in terms of my respective goals for the summer. I learned so much at NIH, and my interest in infertility treatment has blossomed. My experience with health policy related to this field was entirely dependent upon my own initiative. I gained insight into how federal research institutions function, potential areas for growth are in healthcare research (i.e. Big Data), proper leadership skills and how to talk to experts who don’t have MD after their name. I have also decided that a primary research career is not something I want to pursue in my future. Despite the vast amount of information I learned from behind a computer and sitting at conference tables, my true passion for medicine is to be in the clinical setting, working with patients. My glimpse into the REI clinic confirmed my desire to someday be someone’s doctor. This internship experience is invaluable for learning more about research methods to inform my clinical practice, which is probably more important than getting a paper published.  My internship at NIH came to an official end last Friday, although I still have quite a bit of work to do on my manuscript. It was a terrific work experience. My office, Division of Intramural Population Health Research at National Institute of Child Health and Development, consists mostly of epidemiologists and biostatisticians, with a handful of MD's in the mix. Everyone I worked with seemed to have an IQ above 160. They were so on-point with their insight into research methods and statistical analysis. Participating in journal club and attending various research seminars were amazing opportunities to learn about this aspect of health research as we only pick up the bare bones of biostats in medical school. An interesting component of my internship was observing how challenging, yet absolutely necessary, it is to facilitate communication among people from different expertises. I first picked up on this before I landed at NIH, at a briefing on physician payment reform on Capitol Hill. I, along with two of my buddies in the Health Policy track at GWU, trekked over to the Rayburn Building this past spring to listen to a baller panel of policy experts, clinicians and public health people talk about their vision of a healthcare system that transitions away from fee-for-service compensation and is more heavily based on quality and value of healthcare. Their recommendations were carefully thought out. You can read them here. I was curious about how they planned on putting their ideas into action, so I asked the experts during the Q&A session, "What roadblocks do you envision in the implementation of your policy recommendations, and how are you working with lawmakers to make your vision of healthcare reform, a reality?" Okay, my actual question was not that eloquent. I was super nervous. I muttered something that hit those points though. Their responses were not what I expected. The Brookings Institute fellow stated very frankly that implementation was a shortcoming of their recommendation, and something that required more delving into. I was kind of shocked, because here we have these experts spewing knowledge bombs on healthcare reform, but no one knew how to actually implement the ideas. At NIH, I had the opportunity to listen to an international research team's presentation on maternal healthcare in Argentina. I listened to the Dean of the Public Health School at Tulane and researchers at Argentina's premier maternal-child health epidemiology program discuss their ongoing projects in South America. At the end of their presentation, I attended a Q&A session and I asked my question again, this time saying "How will you work with lawmakers to implement some of the research outcomes of your public health work?" I specifically asked the Tulane Dean about his experience working with Bobby Jindal and other New Orleans and Louisiana government officials. He emphatically responded that he does not work with the governor. The Dean and the public health experts admitted that collaboration with lawmakers was seriously lacking, and noted that this was something that needed to be improved upon. I left both the global health seminar and the Capitol Hill briefing with an unsettling feeling. I was impressed by the experts' expertise in their respective fields, but could not comprehend how implementation of their findings was completely omitted from their research process. What is the point of publishing a paper about efficacy of one drug/treatment plan versus another, without informing doctors about the results? What good is performing a study that examines the water quality of various sources without informing government officials about the disparities? Research without implementation is useless. I see a huge potential for improved, streamlined communication among public health experts, policy makers and clinicians in order deliver the most current evidence-based medicine and create an efficient healthcare system. I definitely see myself getting involved in this area in the future. Oh and I also did a pretty cool research product on semen analysis. If you're a fan of epidemiology, infertility treatment or just love semen, check out the snapshot of my poster below. 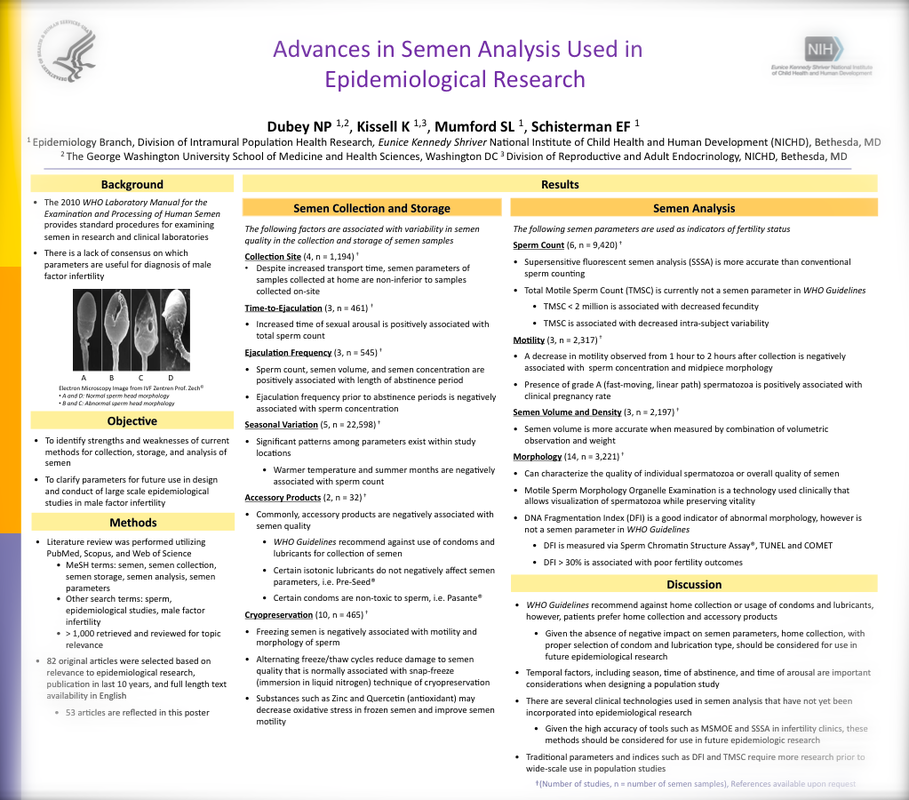
Guantanamo Bay Detention Center currently houses 166 men. All of them are there because they are believed to be threats to the national security of the United States. Few have been formally charged with crimes. In February, several detainees began protesting their detainment by participating in a hunger strike. Earlier this month, as many as 106 prisoners were participating in the hunger strike. In order to prevent any of the detainees from starving to death, the Department of Defense issued orders for the medical staff to forcibly insert feeding tubes into the hunger strikers via their nasal passages. Currently, 44 prisoners undergo this procedure twice a day. Mos Def participated in a voluntary demonstration to illustrate the gruesome nature of this practice. (Thank you, Divya K. for telling me about this video.) He asked to stop the procedure mid-way because he could not tolerate the pain. This video did not make the medical staff at Guantanamo happy. The medics attest that the feeding process is not that bad, and that nobody cries or vomits. One of the nurses is so upset with this YouTube stunt that he went as far as telling Reuters that he was going to delete Mos Def off of his iPod.
After thinking about their comments for a moment, one begins to realize that everyone involved in force-feeding is numbing themselves to the harsh reality of the procedure. The prisoners have grown accustomed to the painful and uncomfortable nature of the procedure. The medical personnel don't want to acknowledge any of the core ethics or peripheral implications of their actions. They justify the force-feeding by convincing themselves that they are providing a benefit to the prisoners by keeping them alive. I'm going to take a moment to say that I don't mean to be disparaging towards military medical personnel who risk their own personal safety to provide for the medical care of American troops and local populations where they are stationed. The medics at Guantanamo are following orders from the DOD. They have no choice but to carry out the procedures they were ordered to perform. My point is that no healthcare provider should be carrying out this procedure. An editorial written in NEJM explains the ethics behind this more eloquently than I ever could. The supporting evidence of Annas' argument and other medical groups' opposition to force feeding are existing medical ethical guidelines, peaceful nature of hunger strikes, and role of medical personnel in carrying out political will of the government. I didn't start to pay attention to how healthcare is delivered in the American penal system until I listened to my friend, Jeremy Levenson's senior thesis presentation about the role of physicians in the Attica Prison Revolt of 1973. The history of what happened in Attica is complex, and I don't want oversimplify the facts, but basically what happened is that prisoners began to protest the inhumane conditions of the upstate New York prison, and successfully overpowered the guards and revolted. The uprising was met with with bullets from the state, and most of the injured prisoners did not receive proper medical attention. Doctors were not sent in because of obvious safety concerns, but Jeremy's thesis points out that the prisoners called for help, and that there were a handful of physicians that wanted to go in to deliver medical care, but were not allowed to. As I reflect on the central question that Jeremy's thesis addressed, which was "Where were doctors when thousands were injured inside the prison gates of Attica?" and juxtapose the role of medical personnel in Guantanamo, the necessity of doctors to function independently of the state becomes abundantly clear. In Guantanamo, medical personnel are being used to maintain the indefinite and unjust detention of unconvicted persons. In Attica, doctors were prohibited from treating many wounded prisoners and permitted over two-dozen prisoners to die due to neglect. Despite their past actions, every prisoner is a human being. Doctors should have no active or passive role in reinforcing the power of the state to dehumanize human beings. Check out this TedEd video about synesthesia. In the video, Dr. Cytowic, neurologist/freelance writer/Renaissance man, narrates, "Synesthetes have two or more senses hooked together. A synesthete might not only hear my voice, but also see it, taste it, or feel it as a physical touch." The short clip beautifully weaves sleek animation, creative imagery and very legit scientific info. Definitely worth a watch even if you know quite a bit about synesthesia. Dr. Cytowic is my mentor for a small group course in patient-interviewing. I got a chance to review the script and make some revisions before he recorded. Pretty sure none of my edits made it in. Whatevs. Are you one of the 4% of people that experiences synesthesia? If so, please allow me borrow your brain. A Washington Post investigation reveals that certain specialists in medicine receive an inordinate amounts of compensation for procedures they perform. This is not new news. What's interesting about this report is the logistics of how price-setting is done. Doctors self-report how long it takes to perform certain services to the AMA, the main lobbying group for physicians, The compensation is determined by negotiations between the AMA and Medicare. The math turns out to be quite fuzzy, as the Post points out, with some physicians earning pay for 26 hours worth of work done in just one day.
It's not just colonoscopies that are driving up the price of healthcare in our country. A recent report by The New York Times illustrates how much maternal health care costs in this country. When one considers that women having been giving birth since the dawn of mankind, but it costs, in 2012 in the United States, $30,000 to give birth through vaginal delivery and $50,000 to cut the baby out via C-section, it is abundantly clear that healthcare costs are spiraling out of control in America. These negotiations between the AMA and Medicare, on how much procedures are supposed to cost, are just as mysterious as negotiations between healthcare practices and insurance groups, which end up determining how much procedures actually cost for the patient. What we end up having is multiple parties with tangible financial incentives, determining how much medical services cost for patients. Prices end up varying across town, and throughout the country. This is shady business. In attempt to learn more about healthcare finance, I asked the simple question, "How much does a visit to the doctor's office really cost?" when I was working with my clinical preceptor one day. He introduced me to a helpful woman in the billing office who demonstrated to me what she does. She verifies the ICD-9 codes (Medicare billing codes) that the doctor enters with the physician's summary of the patient visit and sends that information to another business office. When I inquired about how much specific services cost, and about the breakdown between out-of-pocket costs and what's covered by insurance, I hit a wall. The person in the other business office explained to me that that sort of information is a result of negotiations between the healthcare facility's CEO, business office, legal counsel and the insurance companies. That information is withheld from the healthcare practitioners so that they are deterred from making decisions based on costs. For more information on negotiations between hospitals and insurance companies, like how much leverage hospitals/insurance companies have and a general overview of contract agreements, check out this out. I'm determined to learn more about medical billing. I'm sure most doctors have somewhat of an idea of the costs of services they are providing, but as a medical student, it's important for me to learn about the exact prices of services that I'm going to one day offer. If I'm ordering lab tests, diagnostic imaging, referring patients to specialists or prescribing expensive medicines- I need to know how much that costs. As a responsible physician, I want to offer affordable treatment plans and explain healthcare options to my patients by presenting them in simple terms of costs and benefits. This stuff is complicated. If you have any leads on useful resources, please let me know. |
NeilHealthcare. Business. People. CategoriesArchives
November 2015
|
 RSS Feed
RSS Feed

{kind=link}